Dr Alan O’Rourke, revised by Nick J Fox
Introduction
In this unit, we will build on the discussion from units 2 and 3 on education and revalidation, and explore the issues of measuring performance and how to deal with underperformance. We have also looked at accountability, to patients through the complaints procedure, in keynote 5. But first of all, I have to re-introduce the shocking fact (mentioned in unit 3) that half of all practicing doctors have below average performance! (see Figure 6.1)
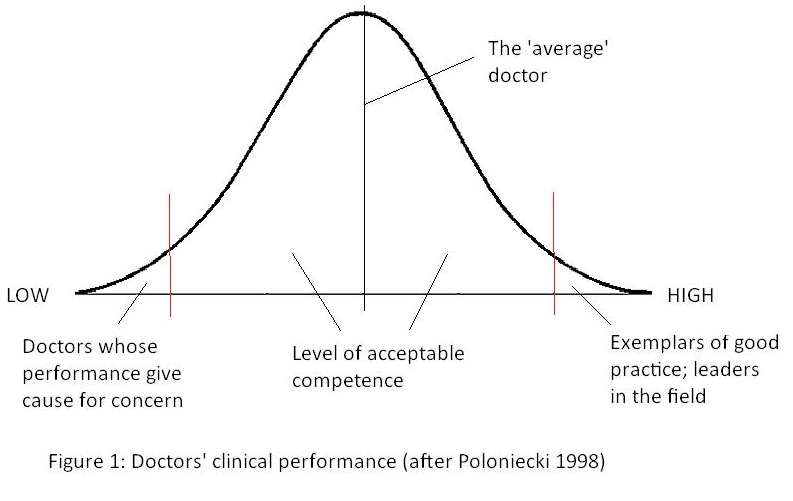
We have already discussed how re-validation, by demonstrating that individuals are keeping up to date and engaging in effective continuing professional development to improve clinical performance, should move this curve to the right and ensure that all practitioners work up the scale – even those saintly characters already at the upper tip! However, the first and more pressing task for re-accreditation is to detect those at the extreme left, offer them remedial education, and if they decline that to remove them from practice. Traditional referrals to professional bodies practicing self-regulation, have proved blunt instruments, resulting in censure not prevention, and backlogs of work.
Clinical governance and accountability
Traditionally, quality in health care depended on the integrity of doctors and nurses, often rooted in the philosophy of the religious orders from which hospitals had grown. Once public money was applied to the relief of suffering, first through the old system of Poor Law infirmaries, later through state services, the issues of probity and value for taxpayers’ money became added parameters in assessing ‘quality.’
In due course professional colleges and regulatory bodies like the General Medical Council (GMC) set standards, which an individual needed to demonstrate in order to commence professional practice. In the 1980’s, healthcare managers attempted to apply Total Quality Management (TQM) to the NHS, largely using models from industry. At the time, patients still trusted these clinicians far more than politicians or managers: the clinicians were largely able to reject these initiatives as bureaucratic exercises, more concerned with cost-effectiveness than clinical care.
Some doctors may in the past have considered themselves answerable only to the GMC and possibly God. But, in today’s climate, healthcare has many stakeholders. The NHS consumes a sizeable chunk of public expenditure and impacts on the lives of all citizens. So, the service and all who work in it must be accountable to those stakeholders.
|
Reflective exercise: Who are ‘stakeholders’ in the NHS? What mechanisms does the NHS have to demonstrate accountability to those stakeholders? |
Identifying and addressing poor performance is part of clinical governance, and chief executives of Trusts, through their ‘duty of quality’ must ensure that their organisation has adequate mechanisms in place to monitor performance. In the last few years, there have been several high profile cases of defective care, and in some of these, the enquiries suggested suspicion of under-performance for years before.
Traditional measures like professional self-regulation and NHS Procedures have clearly failed to protect patients. In the light of these events, the Government has determined to make Trusts more accountable for the actions of their senior clinicians, through processes like appraisal. This delivered a mandate to implement an explicit policy of quality improvement, and ‘levelling up’ to ‘best practice’ in the NHS.
Parallel with clinical governance is corporate governance, introducing the idea that public bodies are not laws unto themselves. They have responsibilities to the wider community of stakeholders to justify decisions and account for resources. As applied to the NHS, corporate governance requires a balance between the freedom of the management to direct and accountability for its actions. We are also now seeing the emergence of research governance, which should provide tighter mechanisms for ensuring that research projects adhere to ethical and other standards.
Performance
Allied to clinical accountability is performance: efficient use of your time and the resources you have control over, to maximise benefit to the health service. Traditionally this has been expressed as productivity: numbers treated or finished consultant episodes. The danger here is that you end up counting events rather than effective interventions: the revolving door approach of patients whizzing through the system so rapidly, that they are bound to be back soon, for another rush job. But, in the future performance should be more closely linked to quality: not just ‘how many things are we doing?’ but ‘how well are we doing things?’
There is a substantial literature on performance management in the private sector, but as yet little on organisations like the NHS. Traditionally, those who worked in the NHS were public spirited individuals, whose professional ethics included ‘doing the best for the patients’ but with little concern (or time!) for quality monitoring. Slowly, concepts like audit were introduced and after the 1990 reforms there were new levers: quality improvement would be driven by incentives like the purchaser-provider split and the internal market, with money following patients.
What is good practice and what is ‘under-performance’?
Within healthcare, there is a huge range of how practitioners manage clinical problems and the results they achieve. Much of this variation does not in itself indicate poor standards: methods may be tailored to local resources and preferences; outcomes are dependent on case-mix and local socio-economic factors. But, concern, at differences in the rates of applying certain treatments and interventions and variations in outcomes across the country, is at the root of the desire to reform the health service, and to level provision up towards ‘best practice.’ However, devolution of decision making to Strategic Health Authorities, PCTs and possibly in the future foundation hospitals, may create new variation. The alternative is rigid central direction about what will be provided, but that will smother local initiative and enterprise. One way of solving this problem may be to insist that all health organisations still have to produce objective information on performance indicators, the so-called ‘traffic light approach.’ Those doing well (green lights) will be rewarded with more autonomy to develop their successful innovations; those showing amber or red will be helped to learn from centres of excellence.
| Reflective exercise Why do standards of health and healthcare vary across the UK? Is all variation ‘bad’? When does such variation become ‘under-performance’? |
The GMC has guidelines on what is good clinical practice. However, defining when a practitioner’s failure to reach these levels represents bad luck, case-mix or lack of care remains problematic. We may use terms like ‘under-performance’ or ‘doctors whose practice gives cause for concern’ for such cases, although these seem to be overlapping but subtly different terminologies here.
- Under-performing clinicians: suggests there is a minimum professional standard, which a practitioner has fallen below. Establishing these standards may be rather arbitrary (at least initially until organisations gain confidence in refining and using these tools), but once these standards are established, this becomes an objective measure.
- Clinicians whose performance gives cause for concern: this is more subjective: ‘concern’ is not defined, but may come from fairly subjective sources (‘His practice does give me some cause for concern.’) It suggests more a process of investigation: the clinician may be practicing competently, but factors like case mix may make their outcomes look poor. Concern suggests the suspicion, rather than the proof, of under-performance.
And possibly a third group:
- Dangerous practitioners: who upon discovery and assessment are so bad as to require immediate action in terms of GMC referral or suspension. There must be some mechanism of detecting this category quickly, or the public will decide the whole process is window dressing. However, this does not resolve the question of where substandard performance is ‘disadvantaging’ patients compared to putting them at risk (e.g. substandard secondary prevention after a cardiac event puts the patient at risk of dying sooner than they need from a recurrence.) All doctor may have isolated incidents of less than ideal performance in their practice, for may reasons, but the main distinguishing feature of this group is recurrent deficits of care across many aspects of their work.
Under-performance can involve any of the following aspects of professional life:
- Conduct
- Failure to discharge contractual obligations
- Poor standards of clinical care
The first two, at least for secondary care, are usually dealt with through existing employers’ disciplinary procedures. The third problem can be handled by local assessment groups, but some cases of gross defects of care may need immediate action at GMC level.
Underperformance and patient safety
As part of the development of clinical governance, a government consultative paper Supporting Doctors, Protecting Patients (Department of Health, 1999) reviewed NHS procedures for dealing with clinical underperformance.
The report recognised the general high quality of clinical care, despite the many challenges of a rapidly evolving healthcare system. Among a population of 90,000 odd registered medical practitioners in the UK, only tiny numbers were subjects of investigations into their clinical competence:
- About 6% of senior hospital staff over a five year period.
- 1-3 consultants per Trust.
- 3-5 GPs for each of the old Health Authority areas.
- 30-40 HO s / SHOs (referred to post-graduate deans for health or performance issues).
The consultative paper accepted the principle of self-regulation, but suggested that it needed certain reforms for the twenty-first century, to develop greater accountability to the public and the Government, and explicit standards for acceptable conduct and clinical competence. It proposed compulsory appraisals for all doctors working in the NHS with a comprehensive programme of training for those doctors involved in carrying out the appraisals. The new model would need to deliver:
- Protection for patients from sub-optimal care.
- Earlier detection of doctors with competency, health or conduct problems.
- Restoration of public confidence.
- Responsiveness to patient concerns, without making the process too difficult for them to negotiate.
- Regulation by explicit and widely disseminated criteria, based on standards of conduct, performance and ethics.
The consultative paper favoured moving away from a reactive disciplinary model, and towards a pro-active remedial one. Appraisal should be comprehensive and compulsory for NHS medical staff – junior and senior hospital staff, GPs and locums.
The process should be linked to re-validation, in a positive pro-active way, aimed primarily at consolidating and improving their skills, and only secondarily at identifying and remedying poor performance. Appraisal should also be integrated more closely with professional education and doctors in training, should receive proper supervision from senior staff, with appropriate rather than expedient, delegation of tasks.
The paper suggested that various models of preventing and detecting under-performance should be explored for use in the NHS such as:
- Pre-employment checks: especially for peripatetic locum staff, such as a log book of all their posts or the American national ‘credentialing’ system, which would cover qualifications, licensing and any outstanding complaints against each doctor.
- Surveillance of clinical data, possibly linked to practice or unit inspection (good method in theory, but may be impractical until better clinical data capture systems are in place).
- Observation of clinical skills, including simulation and skills laboratory situations.
Underperformance and whistle-blowing
The GMC has now moved toward a perspective on underperformance that has as its core an aim to assure patient safety. As such, there is responsibility on all clinicians to raise issues of concern about colleagues’ performance.
It offers this flowchart for health care professionals to use to raise concerns about colleagues. It provides a guide for actions and a link to a support line for potential whistle-blowing. Also take a look at this GMS scenario and consider the question posed below.
Reflective Exercise: A Colleague’s Underperformance
View the GMC interactive scenario about how to address underperformance by a senior colleague.
What are the challenges around whistle-blowing on a colleague’s professional underperformance?
Supporting health care organisations to address underperformance.
Responsibility for addressing poor performance now rests with NHS trusts. If health care organisations are to develop rigorous but fair mechanisms for detecting under-performance before patients suffer rather than holding disciplinary sessions when harm becomes obvious, they face various problems. One of the most fundamental is that they need evidence at two quite different levels. To protect patients, a very low level of suspicion should trigger action. However, the organisation is then left with the problem of what to do about the practitioner. Here, where you are ultimately questioning someone’s professional status, good name and livelihood, much more rigorous evidence is needed (your chosen instrument must now have high specificity).
In 2001 the National Clinical Assessment Service was established to support NHS organisations when they have doctors whose practice gives cause for concern. This became part of the National Patient Safety Agency, and then part of NHS Resolution, as a unit known as Practitioner Performance Advice.
The role of this body is to provide expertise to the NHS on resolving concerns fairly, share from learning for improvement and preserve resources for patient care. It offers a range of core services to NHS organisations and other bodies in England, Wales and Northern Ireland such as advice, assessment and intervention, training courses and other expert services. They say on their website:
Most enquiries we receive come from employers or contracting organisations of which the practitioner is working for about whom there are concerns. Contact is usually made by a senior member of staff, such as a Medical Director, a Director of HR or a Head of Primary Care. However, we can receive initial contact from any representative of the employer or contracting organisation, providing they have the delegated authority to act on behalf of that organisation.
They also offer advice to healthcare professionals and are also a point of contact for whistle-blowers.
Interventions to address underperformance
The Practitioner Performance Advice unit offers a range of interventions to clarify and understand the performance of individual practitioners, and provide the healthcare organisation and practitioner with a sound basis upon which to bring the case towards a resolution. They aim to:
- supporting the local management and implementation of timely and fair management solutions to resolve concerns about performance;
- enabling practitioners to return to safe and effective practice, where appropriate;
- helping to ensure public protection and patient safety (PPA website).
They will draft action plans for doctors, dentists and pharmacists who have been identified by their healthcare organisation as needing support to deliver sustained, safe and effective practice. These plans are either remediation action plans, where there is clear evidence identifying performance or behavioural concerns, or return to work action plans – which support a practitioner’s re-skilling and/orreintegration into clinical practice following a prolonged absence for any reason.
They also undertake clinical performance assessments, to provide an independent view on the clinical performance of the practitioner, or to provide information to assist the referring organisation in decisions about the next steps in their management of the case. It is conducted by a clinical assessment visit by a trained team of assessors, and may include a review of patient records, observation of the practitioner’s normal clinical work and assessment of clinical reasoning and decision-making.
Finally, to support the resolution of relationship difficulties between healthcare professionals, the PPA offers assisted mediation, in which two accredited mediators work with the parties concerned to create a mutual understanding of the issues and to find a way forward that enables a more effective professional working relationship. This may include a clinical team review, to identify any barriers to resolving the issues which have been highlighted and to suggest a plan for improving professional relationships.
Conclusion
This unit has focused on one of the key aspects of clinical governance: accountability of health care professionals for their actions. The development of a programme to address underperformance is the converse aspect of continuing quality improvement. We will return to these issues in unit 9, whe we look afurter at patient safety and significant event assessment.
References
Department of Health (1999) Supporting doctors, protecting patients a consultation paper on preventing, recognising and dealing with poor clinical performance of doctors in the NHS in England. London: Department of Health.
Poloniecki J (1998) Half of all doctors are below average. British Medical Journal, 316: 1734-6.
Resources
GMC web page: Raising and acting on concerns about patient safety.
NHS Practitioner Performance Advice website.
Supporting underperforming trainees. A powerpoint by Dr Vinita Mishra.
© WISDOMnet 2019